Reading time: 6 minutes
Jessica Desamero, PhD
Every year, about 40,000 newborns in the U.S. are diagnosed with congenital heart disease, or CHD. About 1 in 4 newborns with critical CHD need major clinical intervention within their first year of life. (1) Stent placement is a common, minimally invasive treatment for CHD overall. But stent treatment options have been limited for infants, until recently.
In 2024, the FDA approved a special stent system developed by Renata Medical, called the Minima stent. Unlike past stents, the Minima stent is specifically designed for infants and is tailored to accommodate for their growth. Throughout 2025, several pediatricians have started to offer this stent to their patients, and its clinical use continues to expand.
What is congenital heart disease and how does it affect the health of infants?
Congenital heart disease is the most common health anomaly in newborns, with a prevalence of 9 in 1000 live births. (2) Newborns with CHD have abnormalities with the structure of their heart, such as holes in the heart’s wall, issues with the amount or location of blood vessels and problems with heart valves; this in turn may keep blood from flowing normally. Some heart abnormalities reduce the amount of oxygen that can be delivered to cells and can cause low oxygen levels in the blood. (3) Some cases do not cause symptoms, but other cases are life-threatening and require treatment in infancy. Symptoms include bluish skin, lips or nails, excessive sleepiness, extended fatigue, heart murmurs and a weak pulse. CHD increases the risk of other serious health conditions, like abnormal heart rhythms, heart failure, pulmonary hypertension, kidney disease and liver disease. (3)
What were the treatment options for infants with CHD, and why were they limited?
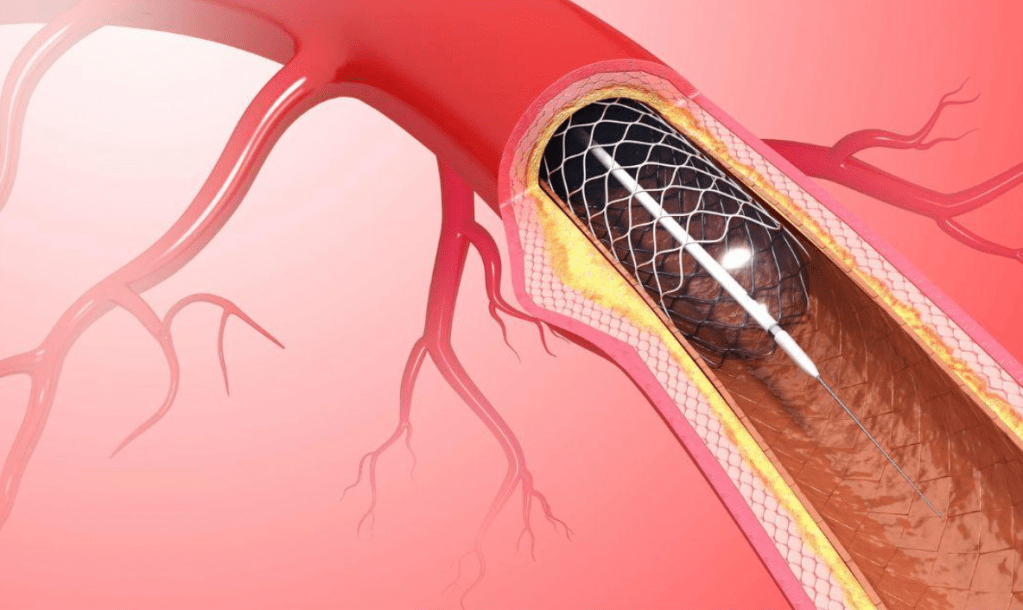
CHD is considered critical when the abnormalities severely limit oxygen flow, and infants with critical CHD require surgery or transcatheter intervention. Transcatheter interventions are minimally invasive procedures that treat CHD by accessing the heart through blood vessels. (4) The main type of transcatheter intervention is placement of a cardiovascular stent, a tiny, expandable wire-mesh tube, to open narrowed blood vessels and restore blood flow.
Since the 1990s, stent placement has been an increasingly common way to treat CHD less invasively. However, stent therapy has remained limited for infants, and few stents have been specifically developed to truly accommodate for an infant’s size and growth. (1) For instance, there is no stent that is specifically designed to be implanted at diameters appropriate for infants and subsequently expanded to adult diameters as the child grows. In addition, there hasn’t been an FDA-approved stent for infants. It’s been common to use off-label adult stents in infants, but this treatment is not ideal for them because of the significantly smaller size of their blood vessels. (5)
What makes the Minima heart stent special?
The Renata Minima stent is the first of its kind to be FDA-approved and specifically designed for infants and tailored to accommodate for their size and growth. (6)
This stent is a cobalt chromium, balloon expandable stent which comes pre‐crimped onto a Minima Delivery System balloon. The unique cell design allows for a wide range of stent diameters, and it is designed to maintain structural integrity and radial strength over the entire range of diameters. (7) At first, the stent has a small enough diameter to be suitable for implantation into infant sized vessels; over time, this stent is able to expand to diameters appropriate for adult-sized blood vessels. (6)
Extensive preliminary testing and evaluation demonstrated the ability of this initially small stent to achieve adult dimensions over time in piglets. (7) A multicenter early feasibility study demonstrated that this stent was safe and effective in treating infants with branch pulmonary artery stenosis, or BPAS, and coarctation of aorta, or CoA. (5) Most importantly, a multicenter pivotal clinical trial, led by Children’s Hospital Los Angeles, further confirmed that this stent was safe and effective for treating PAS and CoA in infants and small pediatric patients. (8) In this study, stent implantation was successful in 98% of patients, and no serious adverse events occurred. Upon, early follow up, no device failure occurred, and the stent remained structurally intact.
How has the Minima stent been implemented recently?
Since its FDA approval in 2024, several leading pediatric hospitals have started to offer the Minima stent for their patients. Hospitals include Children’s Hospital Los Angeles, Nicklaus Children’s Hospital (Miami), Cedars-Sinai (Los Angeles), University of California Davis Health and Cohen Children’s Medical Center.
One baby treated with the Minima stent at UC Davis Health, named Lillian Hodgkin, was one of the most recent success stories, as reported in a news article by UC Davis Health. (9)
Lillian was born eight weeks premature with a genetic condition called DiGeorge syndrome and a congenital heart condition called Type B interrupted aortic arch, where part of her aortic arch was missing. In addition, Lillian had an aberrant left subclavian artery (abnormal distal take off of the artery toward the left arm) and a bilateral patent ductus arteri. In her case, this meant that both left and right blood vessels connecting the main pulmonary artery to the descending aorta, which were meant to be only temporary, failed to close after birth. This, in turn, caused the oxygen-poor blood in her body to flow in the wrong direction, which made her heart muscle weak.
She underwent open heart surgery to repair her interrupted aortic arch, which restored her blood flow. But a follow up echocardiogram showed that her aorta narrowed. Her doctor then decided to use the Minima stent on Lillian, and since the implantation procedure, Lillian became livelier and more energetic. Doctors will continue to monitor her over time and will expand the stent as she grows. But as of now, thanks to the stent, she doesn’t need any more open heart surgeries and is in much better health than before.
Conclusion
Time will tell if these infants experience complications down the line, as it is too early to call. Moreover, Minima is not bioresorbable, and no other bioresorbable stents currently exist for pediatric patients. But bioresorbable stents, which can safely degrade and be absorbed by the body over time, are worth investigating in the future. They eliminate the need for removal surgery, and they reduce the risks of blood clotting, long-term endothelial dysfunction and chronic inflammation. (1)
But overall, the success rates and improvements in conditions in the above cases show the Minima stent system’s true potential as an effective go-to treatment for infants, especially for those who don’t respond to traditional interventions. And so far, the Minima stent has been used in specialized hospitals, but it has the potential for future widespread use.
Header Image Source: from https://www.modernheartandvascular.com/coronary-stenting/
(under a Creative Commons license)
References
- Hatayama, N., Watanabe, T., Yuhara, S. et al. Potential of Biodegradable Stents in Congenital Heart Disease. Biomedical Materials & Devices, 2025, 3, 349–366. https://doi.org/10.1007/s44174-024-00200-5
- Salvatori, G.; De Rose, D.U.; Massolo, A.C.; Patel, N.; Capolupo, I.; Giliberti, P.; Evangelisti, M.; Parisi, P.; Toscano, A.; Dotta, A.; et al. Current Strategies to Optimize Nutrition and Growth in Newborns and Infants with Congenital Heart Disease: A Narrative Review. J. Clin. Med, 2022, 11, 1841. https://doi.org/10.3390/jcm11071841
- Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/21674-congenital-heart-disease
- Mayo Clinic. https://www.mayoclinic.org/tests-procedures/transcatheter-aortic-valve-replacement/about/pac-20384698#:~:text=During%20transcatheter%20aortic%20valve%20replacement,watched%20carefully%20after%20your%20treatment.
- Berman, Darren P, et al. “Results of the Multicenter Early Feasibility Study (EFS) of the Renata Minima Stent as Treatment for Branch Pulmonary Artery Stenosis and Coarctation of Aorta in Infants.” Catheterization and Cardiovascular Interventions, vol. 104, no. 1, 12 May 2024, pp. 61–70, https://doi.org/10.1002/ccd.31074.
- Renata Medical, Minima stent website page. https://www.renatamedical.com/?gad_source=1&gad_campaignid=21743788732&gbraid=0AAAAA-Qcwzeme30P0QWDQFGmd2vHEgCmJ&gclid=CjwKCAiA-__MBhAKEiwASBmsBKgNCuuxStmBpwLca6XB1sHHELVyjdn3HTGuFmqT4AMFZ9JQgkJtFRoCae0QAvD_BwE
- Zahn EM, Abbott E, Tailor N, Sathanandam S, Armer D. Preliminary testing and evaluation of the renata minima stent, an infant stent capable of achieving adult dimensions. Catheter Cardiovasc Interv. 2021;98(1):117-127. doi:10.1002/ccd.29706
- Sullivan, Patrick M., et al. “Multicenter Pivotal Trial of the Minima Stent for Vascular Stenosis in Infants and Young Children.” Circulation: Cardiovascular Interventions, 10 Oct. 2025, https://doi.org/10.1161/circinterventions.125.015618.
- Tomiyoshi, Tricia. “Infant Is First in Region to Get Innovative Stent That Grows with Her into Adulthood.” News, UC Davis Health, 5 May 2025, https://health.ucdavis.edu/news/headlines/infant-is-first-in-region-to-get-innovative-stent-that-grows-with-her-into-adulthood/2025/05. Accessed 27 Feb. 2026.

Leave a comment